6 minutes
Published: April 2024
At the end of 2022, 1,958 CMPA members were general surgeons (Type of Work 83). The graph below compares the 10-year trends in general surgeons’ medico-legal experiences with those of all surgical specialties.
What are the relative risks of a medico-legal case for general surgeons?
- General surgeons, College(n=1,456)
- General surgeons, Legal(n=980)
- All surgical specialists, College(n=7,159)
- All surgical specialists, Legal(n=4,350)
Between 2013 and 2017, the rates of College complaints1 and civil legal actions were higher than those for all surgical specialties. More recently, rates of both College complaints and civil legal actions were close to those of all surgical specialties.
What are your risk levels regarding medico-legal cases, compared to other general surgeons?

| No case |
60.7 |
| 1 case |
25.7 |
| 2-4 cases |
11.9 |
|
| 5 cases or more |
1.7 |
| No case |
88.2 |
| 1 case |
10.4 |
| 2 cases or more |
1.4 |
|
In a recent 5-year period (2018 – 2022)2, 25.7% of general surgeons were named in 1 new medico-legal case (legal action, College or hospital complaint), 11.9% were named in 2 to 4 new cases, and another 1.0% were named in 5 or more cases.
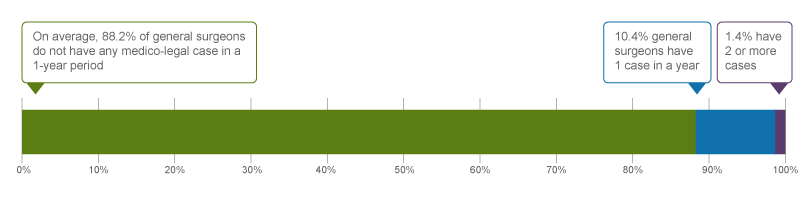
Annually, 10.4% of general surgeons were named in 1 new medico-legal case, an additional 1.4% were named in 2 or more new cases on average across this 5-year period2.
The following sections describe the findings based on the 795 civil legal cases, College, and hospital matters involving general surgeons with peer expert opinions that were closed by the CMPA between 2018 and 2022.
What are the most common patient complaints and peer expert criticisms?3 (n=795)
| Deficient assessment |
46 |
20 |
| Diagnostic error |
31 |
25 |
| Inadequate monitoring or follow-up |
26 |
13 |
| Injury associated with healthcare delivery |
23 |
20 |
| Inadequate consent process |
21 |
15 |
| Failure to perform test or intervention |
21 |
16 |
| Communication breakdown with the patient |
18 |
10 |
| Unprofessional manner |
15 |
4 |
| Insufficient knowledge or skill |
14 |
11 |
| Poor decision-making regarding management |
14 |
6 |
Complaints are driven by the perception that a problem or medical issue occurred during care. These complaints are not always supported by peer expert opinion. Peer experts may not be critical of the care provided, or may have criticisms that are not part of the patient allegation.
There can be more than one criticism per case. For example, the injury associated with healthcare might be the consequence of a deficient assessment which also involved the failure to follow up on a test result.
What are the most frequent interventions with peer expert criticism? (n=795)
- Cholecystectomy (laparoscopic, converted, open approach) (58)
- Endoscopy, with or without biopsy (colon, esophagus, stomach) (55)
- Bowel resection (47)
- Hernia repair (37)
- Bariatric surgery (22)
- Appendectomy (16)
Intervention frequencies among medico-legal cases are likely representative of general surgeons’ practice patterns and do not necessarily reflect high-risk interventions.
Peer expert criticisms
- Deficient assessment
- Inadequate documentation
- Delay or failure to perform test or intervention
- Inadequate consent process
- Inadequate monitoring or follow-up
- Insufficient knowledge/skill
Out of the 795 cases, 160 patients suffered an injury during an intervention. For example:
- Bile duct or bowel injury during cholecystectomy
- Bowel or duodenum injury during endoscopy
- Ureter injury during bowel resection
In addition, 17 patients were noted to have an accidentally retained foreign body post-intervention.
What are the top factors associated with severe patient harm4? (n=795)

Patient factors5
- Age 55+
- ASA status 3 or above6
- Risk factors associated with the need to convert from laparoscopic to open approach (e.g. tissue adhesion, previous history of surgery, obesity)
Provider factors7
- Deficient patient assessment
- Poor clinical decision-making (e.g. failure to convert from laparoscopic to open approach)
- Inadequate patient monitoring or follow-up
Team factors7
- Communication breakdown with nurses
Risk reduction reminders
The following risk management considerations have been identified for general surgeons.
Pre-operative
- Review patient information prior to surgery to ensure that relevant risk factors, comorbidities, past history and any changes since initial evaluation are taken into consideration.
- Ensure the consent discussion includes clear and accurate explanations of the risks and benefits of the proposed procedure or therapy and post-operative expectations, as well as alternative options. Check for patient and family (where appropriate) understanding, and answer questions. Ensure the discussion with patient is clear, concise, and jargon-free, and provide sufficient time to address any patient questions. Document the discussion details in the medical record.
Intra-operative
- Anticipate the potential for intra-operative injuries by routinely having cognitive pauses, particularly during critical or complicated phases in a case.
- Consider altering technique or consulting a colleague when difficulties are encountered during surgery.
- Document details of action taken to protect vital organs or structures, including surgical techniques, anatomical findings, and variants in the operative note. Also document any difficulties encountered and actions taken to address the issue. For example, document the steps taken to identify the ureter.
Post-operative
- Establish clear roles and responsibilities for post-operative care.
- Create a psychologically safe environment where concerns from all healthcare providers on the team about the post-operative patient, even if ultimately unwarranted, can be shared.
- Provide comprehensive discharge instructions to patients or caregivers, both verbally and in writing, including post-operative instructions, wound care, medications, follow-up care, symptoms and signs to monitor, and guidance on when to seek medical attention. Provide clear information on when and who to contact in case of complications.
Limitations
The numbers provided in this report are based on CMPA medico-legal data. CMPA medico-legal cases represent a small portion of patient safety incidents. Many factors influence a person’s decision to pursue a case or file a complaint, and these factors vary greatly by context. Thus, while medico-legal cases can be a rich source for important themes, they cannot be considered representative of patient safety incidents overall.
Now that you know your risk…
Mitigate your medico-legal risk with CMPA resources.
- CMPA Research:
- CMPA Learning:
Questions?
For data requests, please contact [email protected]
Notes
-
Physicians voluntarily report College matters to the CMPA. Therefore, these cases do not represent a complete picture of all such cases in Canada.
-
It takes an average of 2-3 years for a patient safety incident to progress into a medico-legal case. As a result, newly opened cases may reflect incidents that occurred in previous years.
-
Peer experts refer to physicians who interpret and provide their opinion on clinical, scientific, or technical issues surrounding the care provided. They are typically of similar training and experience as the physicians whose care they are reviewing.
-
Severe patient harm includes death, catastrophic injuries and major disabilities. Healthcare-related harm could arise from risk associated with an investigation, medication or treatment. It could also result from failure in the process of patient care.
-
Patient factors include any characteristics or medical conditions that apply to the patient at the time of the medical encounter, or any events that occur during the medical encounter.
-
The American Society of Anesthesiologists (ASA) Physical Status Classification System is used by physicians to predict a patient’s risks ahead of surgery. ASA status 3 indicates severe systemic disease.
-
Based on peer expert opinions. These include factors at provider, team and system levels. For general surgeons, there is no evidence for any system level factors in the data.
